- Products
-
-

DONJOYTRU-PULL LITE™ KNEE BRACE
-

DONJOY GLOBAL QUICK-FIT SHOULDER IMMOBILIZER
-
-
-
-


Pain in the Butt Series 2: Sacroiliac Joint Pain
“Pain in the butt,” a phrase that we typically use to describe someone or something that is very annoying, but it originated from a sensation of pain that is nagging, irritating, and directly affects our quality of life.
When evaluating patients who come in with the complaint of “a pain in the butt”, there are numerous things that could be causing their pain. Sometimes it is their hip, other times gluteal, or back pain. Sometimes it is nerve, muscle, ligament, and/or joint pain that is causing their discomfort. In this series of blogs I plan to tackle some of the various causes of pain I have seen and treated. This blog’s feature is: Sacroiliac Joint Pain
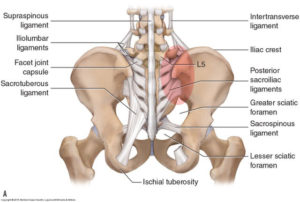 The sacroiliac (SI) joint is a large joint on each side of the sacrum bone at the bottom of the spine made up of two different types of cartilage (synovial and hyaline). The joint is surrounded by very strong ligaments (anterior, posterior (further divided into short/intrinsic and long/extrinsic), interosseous, sacrotuberous, and sacrospinous ligaments). The ligaments make it difficult to dislocate, but these ligaments can develop issues such as sprains, laxity/hypermobility (like an overstretched rubber band), and they are often a missed source of low back pain.
The sacroiliac (SI) joint is a large joint on each side of the sacrum bone at the bottom of the spine made up of two different types of cartilage (synovial and hyaline). The joint is surrounded by very strong ligaments (anterior, posterior (further divided into short/intrinsic and long/extrinsic), interosseous, sacrotuberous, and sacrospinous ligaments). The ligaments make it difficult to dislocate, but these ligaments can develop issues such as sprains, laxity/hypermobility (like an overstretched rubber band), and they are often a missed source of low back pain.
The SI joint ligaments also become more relaxed during pregnancy due to the release of the hormone relaxin (allows the body to accommodate the pregnancy and enable the birthing process). The hormonal changes of menstruation, pregnancy, and lactation can affect the integrity of the ligament support around the SI joint, which is why women often find the days leading up to their period are when the pain is at its worst. The SI joints can also become inflamed with a condition called “sacroiliitis.” The term sacroiliitis refers to inflammation of the SI joint, but most commonly this term refers to an autoimmune inflammatory response of the body causing inflammation of this joint. This can be a part of a rheumatologic condition known as ankylosing spondylitis, and it can also be seen as part of the symptoms of inflammatory bowel disease such as Crohn’s or ulcerative colitis.
Two of the SI joint’s major functions are shock absorption and stabilization (both static and dynamic). The SI joint can also further be divided into an upper pole and a lower pole. The upper pole is typically more involved in static stabilization (ie: sitting or standing still), and is the more commonly injured and painful part of the joint. The lower pole is more involved in dynamic stabilization (ie: walking, running), and is more commonly injured with the superior pole rather than injured by itself.
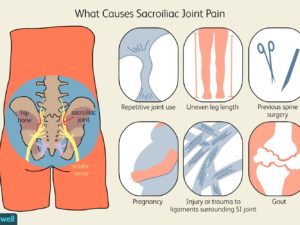 Causes of SI joint pain and dysfunction can include muscle imbalances (notably between the pelvic supporting muscles), trauma (ie: stepping hard onto a locked leg off of a curb), and hormonal changes. It can be seen in conditions of hypermobility such as benign joint hyper mobility and Ehlers-Danlos Syndrome. After having a lumbar fusion patients will often have increased strain on the structures above and below the fusion (post-surgical failed back syndrome), so it is not uncommon to see SIJ pain and instability progressively develop months to years after these surgeries have been performed. Personally I have seen this in athletes where muscle imbalance is an issue. Working many USA Volleyball events I have seen numerous female athletes who will present with acute SIJ pain during competition, often due to the imbalance between their hip internal and external rotators.
Causes of SI joint pain and dysfunction can include muscle imbalances (notably between the pelvic supporting muscles), trauma (ie: stepping hard onto a locked leg off of a curb), and hormonal changes. It can be seen in conditions of hypermobility such as benign joint hyper mobility and Ehlers-Danlos Syndrome. After having a lumbar fusion patients will often have increased strain on the structures above and below the fusion (post-surgical failed back syndrome), so it is not uncommon to see SIJ pain and instability progressively develop months to years after these surgeries have been performed. Personally I have seen this in athletes where muscle imbalance is an issue. Working many USA Volleyball events I have seen numerous female athletes who will present with acute SIJ pain during competition, often due to the imbalance between their hip internal and external rotators.
Symptoms of SI pain may include:
- A dull low back pain felt on one or both sides of the buttock, often in the dimple area
- The pain may become worse and sharp while doing activities such as standing up from a seated position or lifting the knee towards the chest during stair climbing or putting on shoes
- There can be referred pain into the hip, groin, and occasionally down the back of the thigh, but rarely does the pain radiate below the knee
The diagnosis of SI joint pain is often missed as it is not picked up on conventional imaging (XR, MRI, CT), and not all physicians and health care providers are aware of how to diagnose and/or treat it. Typically it is a clinical diagnosis, figured out by a detailed history and properly performed physical examination. In cases of sacroiliitis MRI can be a helpful modality to capture early stages of inflammation and erosion of the joint. Sometimes diagnostic injections into the joint can be used to see if this is the source of the pain.
So we have talked a lot about this condition, so more importantly, how do we treat it?! Treatment typically starts with proper stretching and strengthening exercises, physical therapy, and medications may help alleviate the pain. Osteopathic Manipulative Treatment (OMT) is a manual treatment performed by DO’s that can be a helpful treatment to show the body how to heal itself. For cases that are so uncomfortable that I can barely examine the patient I often will perform a corticosteroid injection (CSI) to calm the area down, allowing the patient to rehab the area. For cases that have become resistant to the above-mentioned therapies and treatments, or for cases that recurrently occur, Regenerative Medicine is often a long-term solution to their chronic problem. Treatments such as shockwave, prolotherapy, platelet rich plasma (PRP), and cell therapy (BMA or ADSC) are able to stabilize the SI joint’s ligaments, allow the joint capsule to function properly (and eliminate pain), and reduce the chances of the pain and dysfunction from ever returning.
physical therapy, and medications may help alleviate the pain. Osteopathic Manipulative Treatment (OMT) is a manual treatment performed by DO’s that can be a helpful treatment to show the body how to heal itself. For cases that are so uncomfortable that I can barely examine the patient I often will perform a corticosteroid injection (CSI) to calm the area down, allowing the patient to rehab the area. For cases that have become resistant to the above-mentioned therapies and treatments, or for cases that recurrently occur, Regenerative Medicine is often a long-term solution to their chronic problem. Treatments such as shockwave, prolotherapy, platelet rich plasma (PRP), and cell therapy (BMA or ADSC) are able to stabilize the SI joint’s ligaments, allow the joint capsule to function properly (and eliminate pain), and reduce the chances of the pain and dysfunction from ever returning.
 For cases that do not respond to the above-mentioned treatments, then pain medicine procedures such as radiofrequency ablation of the nerves surrounding the SI joint, or surgery (typically a fusion of the SI joint), are last resorts.
For cases that do not respond to the above-mentioned treatments, then pain medicine procedures such as radiofrequency ablation of the nerves surrounding the SI joint, or surgery (typically a fusion of the SI joint), are last resorts.
Overall the sacroiliac joint is a common, but very treatable, cause of a pain in the butt. Stay tuned for more of our “Pain in the Butt Series!”
If you or a friend, family member, or colleague is suffering from acute or chronic SI joint pain then reach out to us to see how we can get you moving again!